
Pregnancy is worse than we think
We need more medicalisation of pregnancy, not less

The Global Burden of Disease (GBD) is a huge, comprehensive study of what health conditions cause the most losses to quality and length of life worldwide. Health losses are measured in years of life lost and years lived with disability (reduced quality of life), which are combined into a single measure: disability adjusted life years (DALYs). Disability adjustments are made using disability weights that represent the severity of a condition: values range from 0 to 1 where 0 is perfect health and 1 is dead. All maternal disorders combined have been estimated to contribute about 12.3 million DALYs annually - to contextualise this number, this is a similar burden to liver cancer, slightly more than leukemia.
But nausea and vomiting of pregnancy (NVP) is not recorded in the GBD, despite being maybe the most prevalent cause of ill health in pregnancy. Estimates put the prevalence of NVP at around 70%, although it varies a lot in severity, from mild nausea that comes and goes, through to relentless vomiting that leaves sufferers bed-bound, vulnerable to dehydration and weight loss. The most extreme form has its own diagnosis - hyperemesis gravidarum (HG) - but this has been ambiguously defined for a long time, so prevalence estimates are somewhat unreliable.
We don’t have disability weights for NVP or even HG, but several studies demonstrate substantially reduced quality of life (QOL), worsening with symptom severity. For example, sufferers of moderate NVP have a lower quality of life than people being treated for breast cancer, while severe NVP may be bad physically as suffering a heart attack and as bad mentally as postpartum depression.
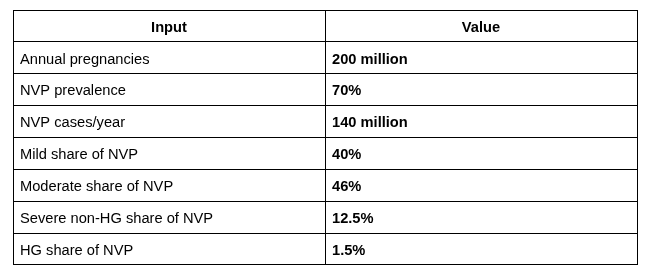
Assuming 200 million annual pregnancies, and given our best estimates of global NVP prevalence, there are about 140 million cases of NVP each year, with most being mild or moderate and 1-2% being HG. The duration of symptoms is correlated with the severity of symptoms but only 50% of cases resolve by 14 weeks gestation, with most resolving by 22 weeks gestation. HG is more likely to last the entire pregnancy (though usually lessens in severity after about 20-24 weeks gestation).
To do a back-of-the-envelope estimation of the global burden of NVP, I’ve used GBD disability weights for plausibly similar conditions: mild gastroenteritis for mild NVP, vertigo for moderate NVP, primary therapy phase cancer for severe, and severe postpartum depression for HG. Average durations of symptoms for the different categories are best guesses based on the NVP literature. Inputs and results are summarised in the tables below.
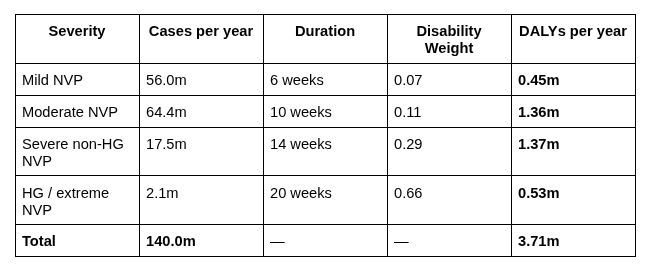
This rough estimation puts the global burden of NVP at 3.71 million DALYs a year. To contextualise this, it’s comparable to that of rheumatoid arthritis (RA) at about 3.1 million, and nearly 4 times that of multiple sclerosis (MS) at 1 million. Both RA and MS are named NIH categories with research funding in the low hundreds of millions each year, plus large charity, academic ecosystems, and private R&D markets (the global RA therapeutics market is worth roughly $25 - $30 billion a year). NVP has no such status. While there is broad spending on maternal health, the focus is very much on reducing mortality and obstetric complications, not on self-resolving maternal conditions like NVP1.
If this figure is in the right ballpark, adding NVP to the list of maternal disorders tracked by the GBD would increase estimates of pregnancy related burden by nearly 30%. And there are other forms of prevalent maternal morbidity not included in the GBD: pelvic girdle pain comes to mind (affects around half of pregnancies, again ranges from mild to severe pain and disability). Ironically, the prevalence of these conditions might have something to do with how overlooked they are: since most pregnant women experience them, they’re “normal” and therefore not of medical concern. Anyone who has approached a GP about their NVP will be familiar with this attitude.
The true health burden of pregnancy is considerably higher than current estimates suggest. Aside from the suffering involved, this is bad for economic productivity, women’s participation in public life, and fertility rates, and we should be doing more to alleviate it.
In recent years, the NVP research agenda has been forwarded in large part due to a single person: Dr. Marlena Fejzo, a geneticist who herself suffered from HG and in 2023, established the etiology of NVP. This breakthrough prompted the development of a new drug that is now in Phase 2 trials; this is a huge deal, as existing anti-emetics offer limited relief to NVP sufferers. Since then, Fejzo and colleagues have identified 10 genes associations with severe NVP, pointing to further biological mechanisms and treatment pathways.